Dear All,
please look at this information (1) from a German Lab from April 3rd already (which later was deleted, but thanks to the wayback-machine, we can still see it):
What they say is that previously 2 target gene sequences from the SARS-CoV-2 were taken for PCR testing, one from the ORF-1 gene and the other one from the E-gene. Only the ORF-1 gene is specific for SARS-CoV-2 while the E-gene is also detectable in OTHER CORONAVIRUSES. Guess what? They are now following the WHO-recommendation and mark a test result as "positive" if only the E-gene is amplified (the non-specific one) but not the specific ORF-1 gene. Also "for simplification" they don´t even let people know which of the targets was positive. In their communication they themselve mark "positive" with quotation marks as if they are aware what bullshit is produced after this change of procedure!
As if this would be not enough, they say that with 2 other SARS-CoV-2 tests from different companies previously they have done a confirmatory test in case the screening test was positive. Now they skip the confirmatory test and mark as "positive" if just the first test was positive. The test targets the non-specific E gene!
Since we know that around 15% of the viruses typical in a common cold are Coronaviruses (2), it is completely fraudulent to do a SARS-CoV-2 test and give a "positive" result, if ANY Coronavirus is detected. This just assures the government that they can maintain people in the fear mode, roll out their surveillance Apps, etc. Disgusting!
If the WHO gave out such a recommendation, that says a lot about their credibility! To check this, I searched for such a doc, and indeed in the WHO-guidance on lab testing for COVId-19 in national laboratories published on the 19th March 2020 (3) they firstly say that "cross reactivity to other coronaviruses can be challenging" but neverheless recommend that in areas "with established COVID-19 virus circulation ... screening by PCR of a single discriminatory target is considered sufficient". One of the targets listed by WHO was the E-gene of which the German lab had said it is NOT specific for SARS-CoV-2.
Also interesting that in addition the WHO says "One or more(!) negative results do not rule out the possibility of COVID-19 virus infection." (3) and in such a case another test run should be done.
It looks like the WHO wants to keep the "pandemic" alive at any costs.
So far this equation "Bill gives money to WHO -> they create the pandemic and nurture it with flawed information -> wordwide vaccination is seen as a must" appeared just too naive for my taste. But now, with the testings so obviously designed to falsely increase the case numbers, I am not sure anymore.
(1) http://web.archive.org/web/20200509151946/http://labor-augsburg-mvz.de/de/aktuelles/geaendertes-befundlayout-der-sars-cov2-pcr-ergebnisse
(2) https://en.wikipedia.org/wiki/Common_cold#Viruses
(3) https://www.who.int/publications/i/item/10665-331501
The original information in German (just in case the web-archive is deleted as well):
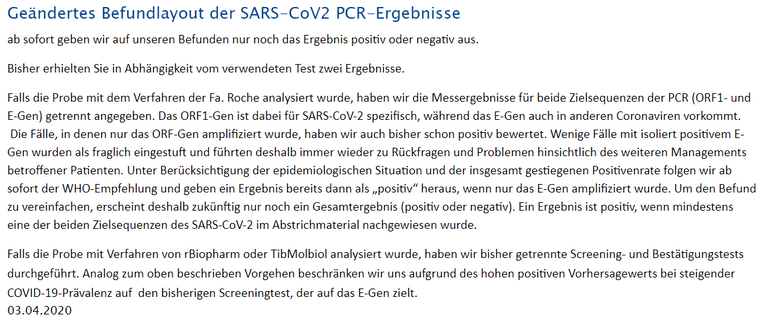
Geändertes Befundlayout der SARS-CoV2 PCR-Ergebnisse
ab sofort geben wir auf unseren Befunden nur noch das Ergebnis positiv oder negativ aus.
Bisher erhielten Sie in Abhängigkeit vom verwendeten Test zwei Ergebnisse.
Falls die Probe mit dem Verfahren der Fa. Roche analysiert wurde, haben wir die Messergebnisse für beide Zielsequenzen der PCR (ORF1- und E-Gen) getrennt angegeben. Das ORF1-Gen ist dabei für SARS-CoV-2 spezifisch, während das E-Gen auch in anderen Coronaviren vorkommt. Die Fälle, in denen nur das ORF-Gen amplifiziert wurde, haben wir auch bisher schon positiv bewertet. Wenige Fälle mit isoliert positivem E-Gen wurden als fraglich eingestuft und führten deshalb immer wieder zu Rückfragen und Problemen hinsichtlich des weiteren Managements betroffener Patienten. Unter Berücksichtigung der epidemiologischen Situation und der insgesamt gestiegenen Positivenrate folgen wir ab sofort der WHO-Empfehlung und geben ein Ergebnis bereits dann als „positiv“ heraus, wenn nur das E-Gen amplifiziert wurde. Um den Befund zu vereinfachen, erscheint deshalb zukünftig nur noch ein Gesamtergebnis (positiv oder negativ). Ein Ergebnis ist positiv, wenn mindestens eine der beiden Zielsequenzen des SARS-CoV-2 im Abstrichmaterial nachgewiesen wurde.
Falls die Probe mit Verfahren von rBiopharm oder TibMolbiol analysiert wurde, haben wir bisher getrennte Screening- und Bestätigungstests durchgeführt. Analog zum oben beschrieben Vorgehen beschränken wir uns aufgrund des hohen positiven Vorhersagewerts bei steigender COVID-19-Prävalenz auf den bisherigen Screeningtest, der auf das E-Gen zielt.
03.04.2020
Wow - they play a very interesting game
Lost your tin foil hat?
Beginning of April was pretty much the height of the epidemic in Germany. So, no wonder they looked for simplification to get as many tests done as possible.
"15% of the viruses typical in a common cold are Coronaviruses"
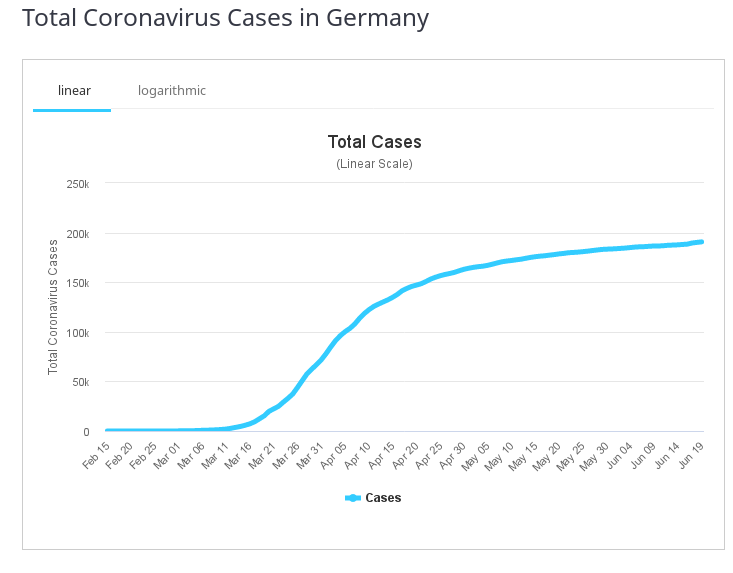
Since the time for colds is almost over by April & it's only 15%, anyway, this won't make much of a difference. & as you can see from the Wuhan virus wave, there is no significant spike in the graph.
"It looks like the WHO wants to keep the "pandemic" alive at any costs."
There is a lot to criticise in the WHO's handling of the pandemic, but this is nonsense. Many tests, particularly from China but also in the USA, showed a lot of false negatives. Hence it was only reasonable to have another test in case of a suspected case.
It is not OK to - just for the sake of running as many tests as possible - provide grossly falsified data!
This cross-reactivity and non-specificity makes exactly the difference! Because due to it you can make out of any virus a pandemic virus, even if it is not more harmful than any other flu virus.
Nope. It's not grossly falsified.
There were not that many other coronaviruses around (at least at the start of April) to be misidentified. & in that moment, 1 or 2 % of false positives don't put any additional pressure on the health system, while quick identification & isolation of cases can lighten the burden.
If anyone still believes that there is no pandemic, then that's just that: belief. & it's useless to argue about religion.
And how can you tell how many other coronaviruses are around?
As has been said before, only some 15% of colds are coronavirus-caused. & since in April the common cold season is virtually over, the probability of a major influence on results is fairly low.
An ad hominem is always good way to start a conversation!
maybe use a better test than pcr if you don't want false negatives or false positives?
How do you know there only were many false negatives?
PCR is about as specific as you are gonna get. I'm not sure what you are insinuating.
pcr is "specific" but has a lot of false-positives and false-negatives - even the Inventor already said that PCR aint good for mass testing - pcr is good when u're in a lab
False positives in pcr tests are usually fairly uncommon, from what I have heard 1-2 % (if the tests were done correctly).
On the other hand false negatives were pretty common, in some tests from China 30% or more (IIRC there were some test batches with about 80%) were false negatives.
Since mostly people with a suspected infection were tested, 1-2% false positives are not too relevant.
It becomes a problem in mass testing, when you eg. test a population in which there is virtually no one infected. But once you do that, you probably have enough testing capacity to immediately have a 2nd test for anyone who tested positive.
what are your sources?
As I said: IIRC.
But for your sake I dug a bit.
The 80% memory came from this: https://www.nationalreview.com/news/china-supplied-faulty-coronavirus-test-kits-to-spain-czech-republic/
Though in the Czech case they perhaps included false positives as well as false negatives in the 80% figure.
That 30% figure goes back to some early Chinese studies, also mentioned here: "Early research out of China stipulated the false negative rate could be around 30%"
For that 1-2% figure, go here: "Large test manufacturers, like Roche, Abbott Laboratories, and Cepheid, all have PCR tests that achieve 100 percent sensitivity and specificity"
So, even better than I thought, but of course, in the field it depends on handling them properly.